Introduction
Hospital cubicle curtains are inexpensive, familiar, and easy to install. They've divided patient bays for decades without much scrutiny. But infection control research is making it harder to overlook what those fabric panels harbor between laundry cycles.
Studies have found MRSA, VRE, and C. difficile on curtains within days of installation. The leading edge — the part staff and patients grab dozens of times per shift — is one of the highest-touch surfaces in any patient room.
Unlike bedrails or IV poles, curtains can't be wiped down with hospital-grade disinfectants without damaging the fabric. That gap in the cleaning protocol is where the infection risk lives.
This article covers what cubicle curtains are, the documented contamination risks they carry, what healthcare facilities should look for in an alternative, and why retractable privacy screens are a proven alternative across emergency departments, multi-bed wards, and outpatient settings.
Key Takeaways
- Cubicle curtains contaminate fast — research shows new curtains can test positive for MRSA and VRE within one week of installation
- Fabric can't be disinfected in place — replacement is the only reliable option, creating recurring cost and workflow disruption
- Non-porous retractable screens wipe down in under two minutes with standard hospital disinfectants
- Portable screens work across settings — ED bays, multi-bed wards, surge scenarios, and outpatient clinics
- Screens cost less over time once curtain replacement cycles and labor are factored in
What Are Hospital Cubicle Curtains?
Hospital cubicle curtains — also called privacy curtains or medical curtains — are fabric dividers suspended from ceiling-mounted tracks. They create partial enclosures around patient beds in shared rooms, emergency bays, and multi-bed wards, providing visual privacy without permanent walls.
Construction Requirements
From a regulatory standpoint, hospital curtains aren't just any fabric. They must meet specific fire safety requirements:
- Flame propagation performance — curtains are typically required to pass NFPA 701 testing, which assesses how quickly a material ignites and spreads flame
- Sprinkler clearance — NFPA 13 requires either an 18-inch clearance below the sprinkler deflector, or a mesh section with openings constituting at least 70% of its area extending at least 22 inches down from the ceiling, to avoid obstructing sprinkler coverage
- Opaque lower section — the solid lower panel provides actual visual privacy; the open mesh section above serves the sprinkler clearance requirement
These aren't optional design features — they're code requirements that facility managers must verify when selecting or replacing curtains.
Aesthetics vs. Material Reality
Nature scenes, abstract patterns, and custom-branded prints have replaced the utilitarian beige of earlier decades. Some facilities have incorporated decorative curtains into patient experience programs.
Aesthetic improvements don't change the underlying material, though. Whether the curtain has a coastal print or a plain blue weave, the fabric structure is the same — and fabric carries the same contamination risks regardless of how it looks.
The Hidden Infection Risks of Hospital Cubicle Curtains
The research on curtain contamination is consistent enough to be taken seriously, even if causation hasn't been definitively established.
What the Studies Show
Laboratory testing published in Infection Control & Hospital Epidemiology found that staphylococci including MRSA survived 1–56 days on polyester privacy drape material, while enterococci including VRE survived 43 to more than 90 days under experimental conditions. These are persistence figures, not proof of clinical transmission — but they establish that the organisms can survive long enough to be a plausible vector.
Field studies tell a similar story:
- Ohl et al. found that 92% of newly placed curtains tested positive for contamination within one week across ICUs and a medical ward — including 21% positive for MRSA and 42% for VRE
- Trillis et al. detected VRE, MRSA, and C. difficile on curtains and confirmed organisms could be transferred via hand contact after touching curtain fabric
- A nursing home study found 22% of 1,521 curtain samples contained a multidrug-resistant organism, with patient-curtain strain matches occurring in a majority of MDRO-positive visits

The Touch-Contamination Problem
The curtain's leading edge — the section staff and patients grab to open and close the enclosure — is handled repeatedly throughout every shift. By everyone. Often without hand hygiene in between.
No authoritative source has counted exact touch frequencies per shift, but the pattern is consistent: the leading edge accumulates contamination faster than almost any other surface in a patient room, precisely because it's treated as a passive furnishing rather than a high-touch surface requiring regular disinfection.
Why Fabric Can't Be Disinfected In Place
Hard surfaces — bedrails, overbed tables, IV poles — can be wiped down with EPA-registered disinfectants during every terminal clean. Curtains can't be treated the same way.
Most hospital-grade disinfectants (bleach solutions, accelerated hydrogen peroxide, high-concentration quaternary ammonium compounds) degrade fabric when applied repeatedly. The EPA notes that most registered liquid disinfectants have been validated for hard, nonporous surfaces — not textiles.
Unless a specific disinfectant has been tested and labeled for a specific fabric at a specific concentration and contact time, applying it to curtains isn't a compliant disinfection strategy. In practice, curtains are either replaced on a schedule or go uncleaned between patient occupancies.
The Replacement Schedule Gap
Infection control guidance calls for curtain changes when visibly soiled and on a regular, facility-determined schedule. In practice, the logistics are significant:
- Curtain must be physically removed from the ceiling track
- Sent to industrial laundry (or disposed of, if single-use)
- A replacement must be sourced and reinstalled
- The full cycle typically spans multiple days
Many facilities lack the staffing or resources to maintain consistent replacement schedules. The curtain stays up, patient after patient, accumulating contamination that can't be verified or audited — leaving a gap that standard terminal cleaning protocols were never designed to address.
What About Antimicrobial Curtains?
Antimicrobial curtains can slow bacterial growth on fabric, but they don't resolve the underlying disinfection problem. A multicenter trial found that one antimicrobial formulation reduced microbial burden while a silver-based alternative did not. Results are product-specific, and no antimicrobial curtain has been shown to eliminate the need for regular replacement.
What to Look for in a Cubicle Curtain Alternative
Not every alternative to fabric curtains is practical in a clinical environment. Three criteria should drive the evaluation:
Cleanability
The primary reason to replace a curtain is contamination risk. Any alternative must solve that problem — not just reduce it. Look for:
- Non-porous surface with no fiber matrix for pathogens to colonize
- Compatibility with EPA-registered disinfectants — specifically bleach-based, quaternary ammonium, and accelerated hydrogen peroxide formulations at label-directed concentrations
- No removal required — cleaning should happen in place, in the same EVS pass as adjacent hard surfaces
Flexibility and Reconfigurability
Healthcare spaces change. Patient volumes fluctuate. Surge events require rapid conversion of open areas. Any alternative to fixed ceiling-track curtains should:
- Deploy and retract without tools or ceiling modification
- Move between departments, floors, or facilities without contractors
- Accommodate different configurations (straight runs, L-shapes, bay clusters)
Fire Safety and Code Compliance
Curtains are subject to NFPA 701 flame propagation requirements and NFPA 13 sprinkler clearance rules. Solid or floor-mounted screens carry different code considerations — they must be evaluated as vertical obstructions under NFPA 13, which may require review by the authority having jurisdiction (AHJ).
Before purchasing, confirm the product comes with documentation covering:
- NFPA 701 flame-propagation test results
- NFPA 13 sprinkler clearance compliance or AHJ review letter
- Listed product data sheets matching your facility's adopted code edition
Why Retractable Privacy Screens Are the Best Alternative
Retractable privacy screens address the curtain's fundamental limitations directly. No construction, no ceiling modification, no multi-day logistics cycles.
The Cleanability Advantage
Rolascreen's privacy screens use inner panels made from non-porous thermally-stabilized polyester film — a smooth, sealed surface with no fiber matrix, no wicking effect, and no pores for microorganisms to colonize. The same class of material is used in blood glucose test strips, reflecting its precision engineering for healthcare environments.
This surface is compatible with the full spectrum of hospital-grade disinfectants:
- Sodium hypochlorite (bleach) at concentrations up to 10,000 ppm
- Quaternary ammonium compounds used in routine daily cleaning
- Accelerated hydrogen peroxide at 4.5% for terminal cleaning
- Alcohol-based wipes for spot disinfection
A complete wipe-down takes approximately two minutes and can be performed in the same EVS pass as bedrails and IV poles. No removal. No transport. No waiting.
Fabric curtain replacement, by contrast, requires physical removal, transport to industrial laundry, and reinstallation over a multi-day cycle — even when the protocol is followed consistently.
Flexibility Without Construction
Rolascreen's Portable Elite units roll on medical-grade casters and require no installation. One staff member can reposition a unit in seconds:
- Retract the screen panel
- Disengage the foot-activated wheel locks
- Roll to the new location
- Lock wheels and redeploy
Screens extend up to 123 inches (10 feet 3 inches) wide and can be configured in straight runs or L-shapes. Multiple units deployed side by side can cover an entire bay cluster or hallway overflow zone. For permanent or semi-permanent installations, wall-mounted models mount flush or extend 18 inches, with professional installation support available.
Total Cost of Ownership
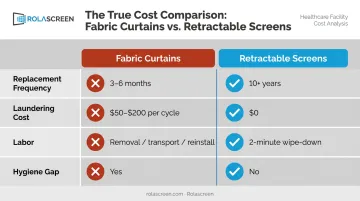
Upfront screen cost is higher than a single curtain. But the comparison changes over a facility's budget cycle:
| Cost Factor | Fabric Curtains | Retractable Screens |
|---|---|---|
| Replacement frequency | Every 3–6 months | 10+ year service life |
| Laundering cost | $50–$200 per cycle | $0 (wipe-in-place) |
| Labor | Removal, transport, reinstall | 2-minute wipe-down |
| Hygiene gap | Yes (between replacements) | No |
Most ED and infusion center deployments reach break-even within two to four years on direct operational costs, before factoring in any reduction in HAI-related expenses. The CDC estimates that HAIs affect approximately 1 in 31 hospital patients on any given day, and the financial burden of each HAI is significant.
Patient Experience and Customization
Rolascreen panels can be printed with custom artwork, calming imagery, or institutional branding. Healthcare organizations including Atrium Health have deployed branded panels in emergency settings. Customization options include:
- Scenic and nature imagery to reduce patient anxiety
- Organizational logos and institutional branding
- Thematic prints tailored to specific care environments
- Custom frame colors to match facility aesthetics
Hard partitions offer none of this. Fabric curtains offer limited versions at best.
Custom-printed panels have lead times of 3–6 weeks; non-printed standard panels ship in 10–30 days.
Where Privacy Screens Outperform Curtains in Healthcare
Emergency Departments and Multi-Bed Wards
High patient turnover and frequent curtain contact make these high-concern environments for curtain-based contamination. Research has documented MRSA and VRE on emergency department curtains, consistent with findings from ICU and general ward studies. Retractable screens that wipe clean between patients eliminate the pathogen-harboring surface entirely. Healthcare systems including Kaiser Permanente, UCSF, and UCLA have adopted retractable screens across departments where infection control and frequent reconfiguration are both priorities.
Surge and Overflow Capacity
During high-census events — flu season, mass casualty incidents, pandemic surges — facilities need to convert non-clinical spaces into private patient areas fast. Portable retractable screens can transform open hallways, waiting rooms, or gymnasium spaces without structural modification.
Regulatory bodies and procurement agencies recognize this need directly:
- FEMA's authorized equipment list includes medical privacy screens for surge scenarios
- ASPR documents alternate care sites as legitimate clinical environments during declared emergencies
- Rolascreen has delivered screens to VA and military facilities and supplied 50 portable units to the Florida Department of Health for disaster shelter deployments
Outpatient Clinics, Therapy Spaces, and Multi-Use Rooms
Physical therapy gyms, counseling rooms, vaccination sites, and infusion centers all share one challenge: privacy needs change throughout the day as patient schedules shift. Retractable screens on casters can be repositioned between sessions in seconds, without the ceiling track constraints that make fabric curtains a fixed infrastructure commitment.
Facilities managing multiple departments can share a fleet of portable units rather than purchasing separate screens for each location — reducing capital costs while preserving flexibility across the building.
Frequently Asked Questions
What are hospital cubicle curtains called?
Hospital cubicle curtains are also commonly called privacy curtains, medical curtains, or hospital curtains. They are fabric dividers suspended from ceiling-mounted tracks used to create partial enclosures around patient beds in shared rooms, emergency bays, or multi-bed wards.
How often should hospital cubicle curtains be changed?
Infection control guidance calls for curtain changes when visibly soiled and on a regular, facility-determined schedule — but no national standard mandates a fixed 6–12 week interval. Many facilities struggle to maintain consistent replacement cycles due to staffing and logistics constraints. This creates a persistent hygiene gap between patient occupancies.
What alternatives exist to hospital cubicle curtains?
Main alternatives include retractable privacy screens (non-porous, wipeable, no ceiling track required), smart glass partitions (high cost, fixed installation), solid folding partitions, and portable room dividers. Retractable screens offer the best balance of infection control, flexibility, and cost for most healthcare settings.
Are retractable privacy screens easy to clean in hospital settings?
Quality retractable screens use non-porous panel surfaces that can be wiped down with standard hospital-grade disinfectants (including bleach-based and hydrogen peroxide solutions) in approximately two minutes. No removal, transport, or reinstallation is needed, unlike fabric curtain replacement.
Can retractable screens help with HIPAA compliance?
Retractable privacy screens can support HIPAA visual privacy requirements in open or shared spaces. HHS confirms that HIPAA does not require private rooms or soundproof walls — physical barriers like screens serve as reasonable safeguards in areas where enclosed rooms aren't available.
Are retractable hospital screens compliant with fire safety codes?
Retractable screens use non-fabric panel materials and are not subject to the same NFPA 701 flame propagation requirements as fabric curtains. Solid or floor-mounted screens should be evaluated as vertical obstructions under NFPA 13. Buyers should confirm compliance with the applicable code edition and authority having jurisdiction before installation.