Transparent barriers are not inherently effective. They become effective when they're correctly designed, properly installed, and consistently maintained. A barrier that ends 16 cm below a user's breathing zone — as documented in NIOSH laboratory research — provides no meaningful protection.
This guide covers what facility managers, healthcare administrators, and operations teams need to know to get barrier implementation right: dimensions, openings, barrier types, installation, and cleaning protocols.
Key Takeaways
- Barrier height and width must extend well beyond both users' breathing zones to block respiratory exposure effectively
- Pass-through openings must stay small and must not align with anyone's face
- Many common disinfectants damage acrylic and polycarbonate — material compatibility matters
- Barriers reduce droplet exposure but don't address aerosol transmission — ventilation support is still required
- Portable and retractable options work well where space configurations change frequently
Why Transparent Barriers Are Used for COVID-19 Prevention
Transparent barriers serve three distinct functions in infection control:
- Intercepting respiratory droplets — particles larger than 5–10 microns that travel in a relatively direct path from speaker to listener during close-range interaction
- Reinforcing distancing — creating a physical boundary even when users instinctively lean in to speak or pass documents
- Reducing sole reliance on masking — particularly in settings where masking is inconsistent, difficult to enforce, or not feasible for users (such as customers at retail counters)
What Barriers Can and Can't Do
The distinction between droplet and aerosol transmission is critical here. Droplets (larger, heavier particles) follow a relatively direct trajectory and can be intercepted by a properly sized barrier. Aerosols (particles under 5 microns) remain suspended in room air and can travel around, above, and beside barriers.
The CDC has explicitly warned that barriers can interrupt airflow and concentrate aerosols in some configurations, which can increase localized exposure rather than reduce it. This means barriers are a targeted tool for direct, face-to-face droplet exposure — not a room-wide solution for aerosol-heavy environments. Ventilation remains essential alongside any partition strategy.
Barriers have been recommended across a wide range of settings, each with distinct sizing, material, and cleaning requirements:
- Hospitals and healthcare clinics (triage desks, reception windows)
- Urgent care and walk-in facilities
- Schools and university administrative counters
- Government offices and public service counters
- Airports and transportation checkpoints
- Retail and commercial counter environments
A hospital triage barrier, for instance, demands different height clearance and disinfection compatibility than a school reception window — which is why fit-for-setting design matters as much as the barrier itself.
Guidelines for Designing and Selecting an Effective Transparent Barrier
Not all barriers on the market are designed to public health standards. Before purchasing, decision-makers need to evaluate four things: dimensions, openings, material, and form factor.
Dimensions and Coverage
The breathing zone — the pocket of air within approximately 30 cm (12 inches) of a person's nose and mouth — is the reference point for every sizing decision. A barrier that doesn't cover both users' breathing zones isn't doing its job.
Key sizing principles from NCCEH physical barrier guidance:
- Height must cover the breathing zones of both the tallest expected standing user and any seated users — a standing customer and a seated cashier can have dramatically different face heights, and the barrier must account for both
- Width should span the full counter or workstation — narrow barriers allow users to lean sideways to speak around them, which defeats the purpose entirely
- NIOSH findings: Laboratory testing found barriers reaching 91 cm above the table and at least 91 cm wide achieved up to 93% reduction in simulated cough particles; a barrier ending just 16.5 cm below cough height provided no significant protection
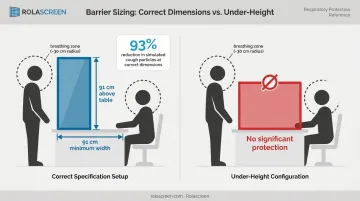
When in doubt, size up. The cost of a slightly larger barrier is trivial compared to the cost of one that doesn't protect.
Openings and Pass-Through Slots
Any opening in a barrier — document slots, payment terminal cutouts, package pass-throughs — creates a direct path for respiratory particles. The rules:
- Keep all openings as small as functionally necessary
- Position slots away from both users' breathing zones — a document slot offset to the side is far safer than one centered directly in front of a seated worker's face
- Never add speaking ports or grates — these create a direct channel through the barrier, routing exhaled air from one user to the other
- Flexible plastic flaps over larger openings are high-touch surfaces and must be cleaned at minimum twice daily
Barrier Type: Fixed vs. Portable and Retractable
| Type | Advantages | Risks |
|---|---|---|
| Surface-mounted fixed | Stable, minimal base gap, preferred for permanent workstations | Less flexible for reconfiguration |
| Hanging barriers | Easy to install | Can swing, leave large counter-level gap, harder to clean |
| Free-standing portable | Flexible, repositionable | Can tip if bumped; requires securing or weighted base |
| Retractable screens | Highly flexible, wipeable, deployable in variable configurations | Requires selection of non-porous, cleanable materials |
Surface-mounted or stable free-standing designs are the preferred configurations in most public health guidance. Hanging barriers carry the highest risk — they can waft air at counter level and leave gaps that undermine the entire installation.
That said, some settings can't rely on fixed installations. Emergency departments, vaccination sites, open-plan offices, and disaster shelters all require barriers that redeploy as needs shift — and retractable screens are built for exactly that.
Rolascreen's retractable screens (available in transparent configurations) use non-porous thermally stabilized polyester film. The material wipes clean with EPA-registered hospital disinfectants used on bedrails and IV poles. The entire surface cleans in the same EVS pass as adjacent hard surfaces, with no separate protocol required.
Safe Installation and Placement Practices
A correctly sized barrier can still create problems if placed or secured improperly. Three installation issues consistently trip up facilities:
- Egress compliance: Under OSHA 29 CFR 1910.37, exit routes must remain free and unobstructed. Barriers positioned across walkways or near emergency exits may violate this requirement — verify placement against local fire and safety codes before deployment.
- Stability of freestanding units: Large freestanding panels can tip when bumped. If fixed mounting isn't feasible, use a weighted base or temporary adhesive anchoring. Wheeled portable units should only be deployed on level floors where the unit will stay stationary during use.
- Bottom gaps: The gap between a barrier's base and the countertop or floor is a real infection control vulnerability — respiratory particles travel along surfaces and through the air. Surface-mounted barriers minimize this gap. Hanging barriers that swing freely or sit well above the counter carry the highest risk for this reason.
Cleaning and Maintaining Transparent Barriers Properly
A barrier that intercepts respiratory droplets becomes a contaminated surface. It must be treated as one.
Cleaning Frequency
- Non-contact barrier surfaces: Clean at least daily
- Touched surfaces (pass-through edges, flexible flaps, any surface users contact): Clean at least twice daily, more often under heavy use or when visibly soiled
Material Compatibility: Where Many Facilities Go Wrong
Standard acrylic and polycarbonate panels are vulnerable to degradation from many common disinfectants. The table below reflects manufacturer testing data:
| Material | Bleach | 70% Isopropyl Alcohol | Quaternary Ammonium |
|---|---|---|---|
| Acrylic (OPTIX) | Compatible (household concentration) | 30% IPA compatible; 70% not established | Compatible at use dilution |
| Polycarbonate (TUFFAK) | Incompatible | 70% IPA compatible | Clorox Broad Spectrum incompatible |
| Polycarbonate (Makrolon) | 10% bleach compatible under low stress | Not reported | Clorox wipes caused stress cracking |

Safe options for most acrylic surfaces include mild soap and water, hydrogen peroxide-based products listed as compatible with the specific material, and disinfectants validated by the sheet manufacturer.
Check EPA List N for antimicrobial efficacy against the virus. That is a separate question from material compatibility with the plastic. Both checks are required.
Why Rolascreen's Panel Material Differs
Rolascreen's Guard sneeze guards use non-porous thermally stabilized polyester film rather than acrylic or polycarbonate. The non-porous structure means disinfectants remain on the surface rather than penetrating the material. That stops the stress cracking and crazing that acrylic panels develop under repeated chemical exposure.
The material is validated for:
- Sodium hypochlorite up to 10,000 ppm — twice the upper bound of the CDC's C. diff sporicidal protocol
- Quaternary ammonium compounds including CaviCide, CaviWipes, and Virex
- Accelerated hydrogen peroxide (Virox)
- Alcohol-based wipes (with care on printed surfaces)
The practical result: the barrier can be wiped in the same cleaning pass as bedrails and IV poles. No separate workflow. No incompatibility risks. After thousands of cycles, there is no visible degradation.
Common Mistakes That Undermine Barrier Effectiveness
Three patterns consistently compromise what barriers are supposed to do.
1. Undersized barriers leave users unprotected. Many commercially available desk shields are too short to cover the breathing zone of a standing user interacting with a seated employee. A barrier that looks substantial from across the room may leave both users' faces entirely exposed during actual interaction. Worse, it can increase complacency around masking and distancing without providing the protection that justifies that trade-off.
2. Treating barriers as a standalone solution creates net risk. Barriers address directional droplet exposure. They do nothing for aerosol transmission, hand-to-face contamination, or respiratory exposure outside the immediate interaction zone. Removing masking, hand hygiene, or ventilation improvements because a barrier was installed introduces new risk rather than reducing it. Barriers are one layer of a multi-part system.
3. Skipping cleaning schedules turns barriers into transmission surfaces. When protocols aren't formally updated to include barriers, barriers simply don't get cleaned. This is usually a systemic oversight, not negligence: cleaning staff work from documented checklists, and if barriers aren't on the list, they're invisible to the routine. Barriers that accumulate respiratory droplet residue become contaminated contact surfaces, contributing to transmission rather than preventing it.
Conclusion
The difference between a transparent barrier that works and one that doesn't often comes down to details that aren't visible at the point of purchase: whether the height actually covers both users' breathing zones, whether the cleaning product is compatible with the panel material, whether the bottom gap is sealed, whether the cleaning schedule was updated.
Facility managers should treat barrier implementation as an ongoing operational responsibility, not a one-time purchase. Key checkpoints to revisit regularly include:
- Coverage fit: Does the barrier still match how staff and visitors are positioned at each station?
- Cleaning compatibility: Are the products being used safe for the panel material?
- Gap seals: Is the bottom edge still flush, or has wear created a bypass route?
- Protocol updates: Has the cleaning schedule kept pace with current public health guidance?
Configurations that made sense during peak COVID-19 response may need revision as staffing shifts or space usage evolves. A barrier that gets installed and forgotten can fail silently — or worse, give staff and visitors confidence that a risk has been addressed when it hasn't.
Frequently Asked Questions
Do plexiglass barriers protect against COVID?
Plexiglass (acrylic) barriers offer meaningful protection against respiratory droplet transmission when properly sized to cover both users' breathing zones. They are less effective against aerosol transmission and must be used alongside ventilation, masking, and hand hygiene for comprehensive protection.
What dimensions should a COVID-19 barrier be to be effective?
Height should exceed the breathing zone of the tallest expected standing user while also covering seated users — accounting for both postures when both occur at the same workstation. Width should span the full counter or workstation surface. The breathing zone extends roughly 12 inches from the nose and mouth in all directions.
Can regular disinfectants be used on acrylic or polycarbonate barriers without damaging them?
Many standard disinfectants, including bleach-based or high-concentration alcohol products, can cloud or crack acrylic surfaces over time. Polycarbonate has its own incompatibilities. Use mild soap and water, or disinfectants specifically validated as compatible with the panel material.
Are transparent barriers still relevant for infection control beyond COVID-19?
Physical barriers remain a practical tool for reducing droplet transmission during respiratory illness outbreaks including influenza and other respiratory viruses. CDC foundational isolation guidance supports glass or plastic barriers at reception and triage as a general respiratory hygiene measure.
What is the difference between fixed and portable transparent barriers?
Fixed barriers are surface-mounted for permanent workstations, providing stability and minimal base gaps. Portable and retractable barriers can be repositioned as needed, making them valuable in emergency departments, vaccination sites, and other settings where layouts shift frequently.
Do transparent barriers eliminate the need for masks?
No. Barriers address directional droplet exposure at face-to-face service points; they don't address aerosols, which can travel around them. Public health guidance consistently describes barriers as one element of a layered approach that still includes masking for close or prolonged contact interactions.